Integration with NCD management is the key to addressing obesity
Policy Insight SERIES on Obesity | 03
Sponsored by

Sponsored by
Integration with NCD management is the key to addressing obesity
Policy Insight Series on Obesity | 03
Jason is 53 and lives with obesity and related chronic diseases.
His general practitioner tells him to “lose weight” but without any services to refer to. His knee pain leads him to an orthopaedic referral, where surgery is suggested, but where he is not informed about how living with obesity links to developing other chronic diseases, such as knee osteoporosis, diabetes, liver or cardiovascular disease. And when he mentions feeling low, he is told to find mental health support elsewhere. Every appointment and conversation is disconnected. No one sees the full picture or treats obesity as a chronic disease that exists within a web of others. He doesn’t know where to go, or who can help.
Jason is exhausted because his care is fragmented, reactive and because there are no opportunities to get management for him as a whole person, only for each disease in isolation. He’s trying his best—but his health is getting worse.
“We have a cluster of diseases that interact together… but health systems are set up around organs and specialties. That’s part of why obesity is so hard to manage.”
Dr. Sara Suliman, Imperial College, Abu Dhabi
Obesity connects the NCDs we treat in isolation
Imagine a car that is solid, reliable and built to last, but only with regular maintenance–regular oil changes, brake checks, and the occasional new set tyres. Look after it, and it will keep running for years.
This is the metaphor for obesity Dr. Sara Suliman from Imperial College, Abu Dhabi, offered at the recent panel discussion on The economic imperative: policy solutions for tackling non-communicable diseases, an Economist Impact event sponsored by Novo Nordisk on the sidelines of Abu Dhabi Global Health Week.
But unlike machines, human bodies are not all manufactured to identical specifications. Not all cars start from the same blueprint. Some have built-in vulnerabilities–genetic predispositions, early-life exposures, or structural disadvantages–that require more than routine care.
Which is why the metaphor must go one step further. We need to stop fixing parts in isolation and start looking at the whole vehicle and its environment to optimise function. Health systems should be designed with the same mindset: to support the body more holistically, across time and circumstance, integrating care across different disease areas.


Obesity connects the NCDs we treat in isolation
“We can't work alone and we can't achieve or tackle obesity or NCDs by one sector. So all of us are responsible for that.”
Professor Haleama Al Sabbah, Associate professor in public health and nutrition at Abu Dhabi University
The human body is not built in silos. Rather, one area often affects another. But if many conditions rarely exist in isolation, why is care delivered as if they do?
The most effective initiatives for preventing and managing NCDs, the true “best-buys”, are those that target the shared drivers of ill health. One of the most common and consequential drivers is obesity. Obesity contributes to the onset and progression of many chronic diseases, including type 2 diabetes, cardiovascular disease, liver disease and certain cancers. Yet despite its reach, obesity is still treated mostly as a standalone risk factor, both in care pathways and in policy.
“Obesity is really what connects NCDs. And you really need to think about how to tackle obesity in a holistic way if you really want to have impact in many other NCDs.”
Dr Simón Barquera, Director of the Nutrition and Health Research Centre at the National Institute of Public Health, Mexico
To tackle obesity—and therefore NCDs—effectively, we need to change how we perceive obesity, and how we manage it in a way that acknowledges what we know about the science of obesity. First, obesity must be recognised as a disease in its own right, and as a strategic entry point for broader NCD prevention, care and policymaking. Second, addressing it requires an integrated, coordinated approach of policymaking and of care that spans across specialties, systems and stages of life. A failure to do both will not prepare us well for the serious economic and developmental consequences of this epidemic.
We’ve long known that integrated care is the answer. But knowing is not the same as doing. So where do we start?
Key elements
Unifying collaboration: Addressing obesity demands a whole-of-society approach, detailing and assigning stakeholders’ responsibilities across government, academia, NGOs and the private sector to ensure accountability, efficiency and impact.
Integrating policy approaches: A “health-in-all-policies” approach embeds health considerations into policies across sectors, such as urban planning, education, and agriculture. This is essential to tackle the underlying social and environmental drivers of obesity, while also ensuring people living with obesity have access to quality care they need.
The playbook for integrated obesity prevention and management is already available
In the last policy insights post, Francesca Celletti, Senior advisor in WHO’s Nutrition and Food Safety Department, said, “there is no one-size-fits-all solution to policymaking around obesity.” Each country will do it differently, but together they are paving the way.
Italy is already showing what bold leadership looks like. In a historic move, it became the first country in the world to legally recognise obesity as a chronic disease, setting a global precedent for shifting how obesity is understood, prioritised and addressed in policy. The landmark law enshrines provision for prevention and treatment. But above all it sends a powerful message of galvanising international attention and encouraging other governments to act.1
Other countries have integrated obesity prevention and management. In France, for example, Centres Spécialisés Obésité (Specialist offer a dedicated, multidisciplinary model. These centralised hubs provide prevention, treatment and long-term management for people with severe or complex obesity, while also coordinating regional care pathways, supporting local providers, and contributing to national training and research.2
We can also learn from how other complex diseases are managed. As outlined in our National Obesity Action Plan Playbook, obesity shares many features with mental health and diabetes. All are shaped by a mix of biological, social and environmental factors. All have a legacy as being stigmatised and oversimplified diseases. And all can benefit from joined-up, long-term care that meets patients in the context of their daily lives.
“We tell people to eat better and walk more, but we do not give them the tools or environment to do those things.”
Dr. Shereena Khamis Al Mazrouei, Director of health promotion and public health programmes, Abu Dhabi Public Health Centre

We need to give people the tools and environment to live healthier for longer. If our surroundings are working against us, even the best intentions of action cannot be realised. This involves looking at other sectors as well. Take urban design: if neighbourhoods are not built with safe pavements, nearby parks or affordable leisure activities, then opportunities for physical activity disappear. We tell people to move, but what if there is nowhere safe or affordable to go?
“Health in all policies is the trigger to make things happen. It is an accelerator. The health sector worked hard for many years; they cannot do it alone.”
Dr. Shereena Khamis Al Mazrouei, Director of health promotion and public health programmes, Abu Dhabi Public Health Centre
That is why intersectoral policy and planning at the system level matters. People need environments that make healthy choices not just possible, but easier, to live their healthiest lives.

Pages from diabetes and mental health prevention and management
“We need to take a step back and speak together. Starting with the problem, treating inequities and managing disease at their origin. If we look long term, we save more.”
Dr. Sara Suliman, Imperial College, Abu Dhabi
Integrated care models from diabetes offer valuable lessons. In Ontario, Canada, the Primary Care Diabetes Prevention Program provided structured lifestyle counselling for people with prediabetes or metabolic syndrome. As part of the province’s broader diabetes strategy, it aimed to reduce disease onset—and succeeded: participants lost an average of 7.5% of body weight in nine months, with modelling suggesting one case of diabetes prevented for every 36 people enrolled.3 In Italy, Diabetes Care Units in the Emilia-Romagna region support long-term management through multidisciplinary hospital-based teams connected to general practice. These units coordinate care across nutrition, mental health, and complication screening, and have been shown to reduce avoidable complications and improve outcomes.4
Similar lessons can be drawn from mental health. Australia’s Headspace Centres offer co-located mental health, physical health, substance use and vocational support for adolescents—all free of charge. Approximately one-third of young people showed significant gains in psychological distress, functioning or quality of life within 90 days of care over a 16-year evaluation period.5 Meanwhile, Brazil’s Psychosocial Care Centres (CAPS) are part of a larger community mental health reform, offering multidisciplinary outpatient services and crisis support together. The increase of CAPS coverage from 2013-2019 is paralleled with increases in outpatient care and reductions in long-stay psychiatric hospitalisations.6
These models provide examples of how integrated, community-based systems for prevention and management may be adapted to help coordinate long-term, person-centred and integrated care for obesity.

Writing our own next chapter in obesity prevention and management
Integrating obesity into national health and development strategies requires political commitment, policy coherence and long-term investment. As countries recommit to frameworks like the WHO Acceleration Plan, they must ensure that obesity policy-making, prevention and management is no longer siloed or treated as an afterthought. Integration must be intentional and supported by robust monitoring and evaluation from the outset to ensure it is sustained.
“Obesity is a long-term trend; you don’t have success in minutes, or even in years. You need at least 10 years of sustainability to see significant changes.”
Martine Laville, Professor Emeritus, Lyon 1 University, France
Imagine Jason again.
But this time, he lives in a world where obesity is taken seriously as a disease. As a result, its prevention and management is integrated into every day health promotion and health care services. He is included actively in his care plan, knows where to go and who to turn to. His care is connected between services and not scattered across them, and most potential complications are caught before they escalate. Jason no longer feels confused or blamed by the system. Instead, he feels supported, seen and in control of his health.
That is the kind of health care system people living with obesity deserve. And integrating obesity prevention and management into NCD care is one major step in that direction.

Audience key take aways
There is a need for all-of-society action on obesity–the solutions do not just lie in the healthcare system.
Position obesity at the heart of NCD prevention–progress on obesity unlocks progress across other major health targets.
A shift in narrative around health system funding to reflect the investment in keeping populations in good health rather than the cost of treating ill health.
We would like to thank the panellists and audience who took part in the discussion at The economic imperative: policy solutions for tackling non-communicable diseases, an Economist Impact event sponsored by Novo Nordisk on the sidelines of Abu Dhabi Global Health Week.
- Buthaina Abdulla Bin Belaila, Head of non-communicable diseases and mental health, Ministry of Health and Prevention, UAE
- Haleama Al Sabbah, Associate professor, Abu Dhabi University
- Sara Suliman, Clinical lead for obesity, genetics of diabetes and endocrinology, Imperial College London, Abu Dhabi
- Shereena Khamis Al Mazrouei, Director of health promotion and public health programmes, Abu Dhabi Public Health Centre
- Dan Beety, Senior director, global obesity policy and public affairs, Novo Nordisk
We will be continuing the conversation at upcoming events around the World Health Assembly and UN General Assembly, and welcome policymakers, advocates and changemakers to join us in advancing obesity on the global health agenda.
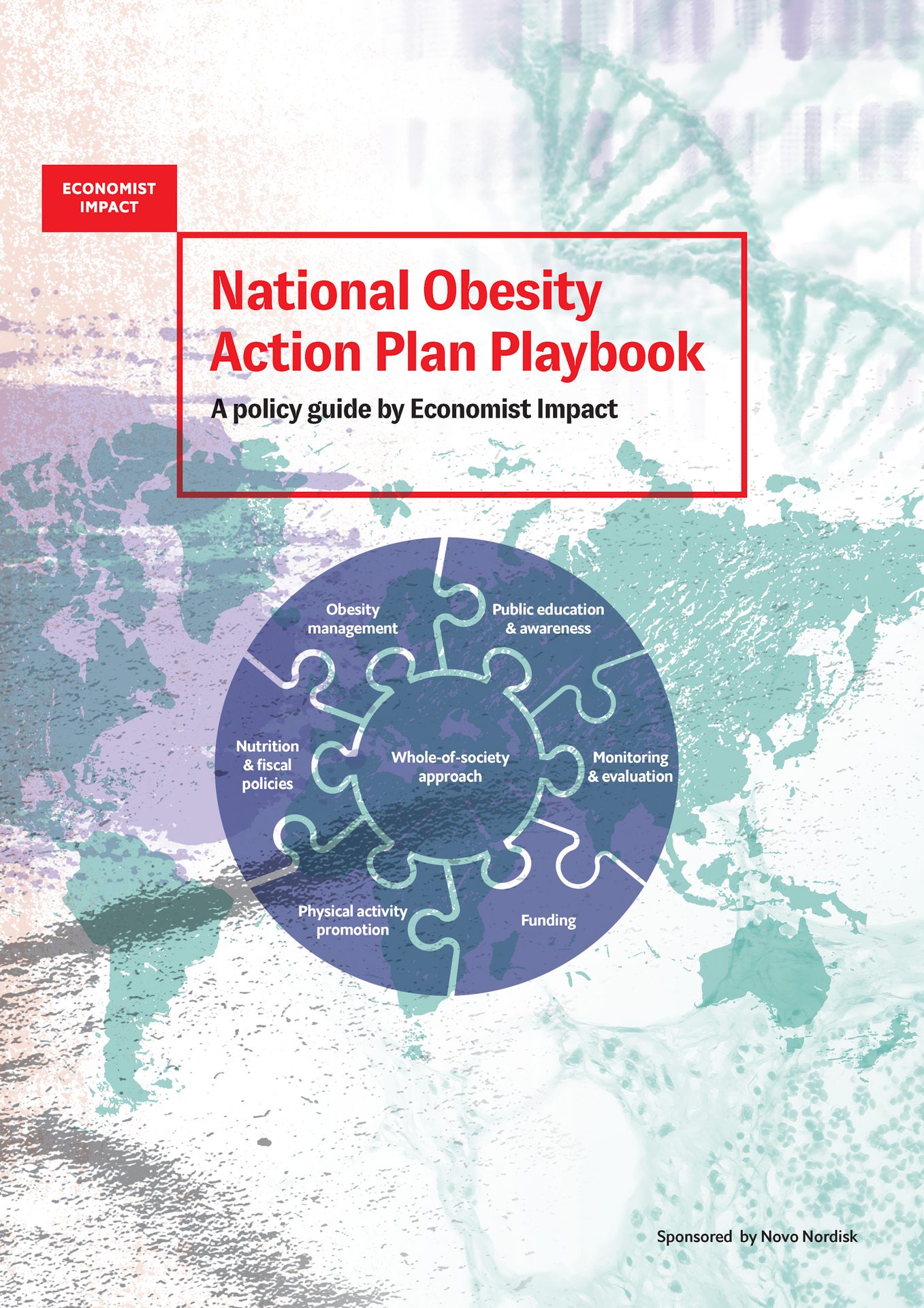
The National Obesity Action Plan Playbook contributes to advancing policy and national action on obesity by providing policymakers with a practical framework for designing and strengthening national strategies to prevent and manage obesity. Drawing on WHO guidance, global expertise, and case studies, it identifies key action areas and highlights best practices for tackling obesity’s systemic drivers through a whole-of-government and whole-of-society approach.